Shoulder Pain
Shoulder pain is the third most common complaint we treat. Though the pain is felt in the shoulder girdle region, more times than not, the cause is not of the shoulder itself, or there’s a secondary contributor to the problem! The pain we feel — whether in the neck, the shoulder(s), or down the arm(s) — is the body’s request for change, not an indication something is broken, needing to be “fixed.” By taking the time to understand the problem and how it behaves, we can apply the right tool for the job — only then can we achieve a solution.
WHAT IT IS
Shoulder pain is most commonly of mechanical nature, e.g., movement, postures, body mechanics. If your shoulder pain changes — for better or worse — with varying movements and positions accompanied by stiffness or loss of range of motion, you likely are suffering from mechanical pain. The question is: is it truly a shoulder problem or is pain coming from a remote location?
Acute shoulder pain is an episode lasting no longer than six weeks, which is more common than chronic shoulder pain lasting longer than three months.
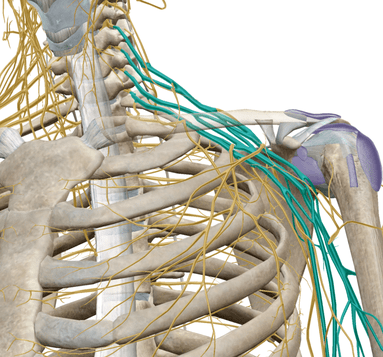
Because the nerve supply to your shoulders and arms stem from the spinal cord within the spinal column, suboptimal cervical spine (neck) mechanics can alter the signals from your brain to the shoulder muscles via nerve pathways. It is not uncommon to experience shoulder symptoms when the neck is the source; in fact, we find it’s the case more times than not!
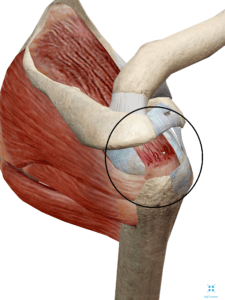
To be crystal clear, we do not correct tears and arthritis. Above are standard labels tagged on patients, which we have successfully treated, regardless of the diagnosis — call it “misdiagnosis” if you will. The problem with these diagnoses is they simply tell you what it is, not how or why it occurred, nor how to correct it. Furthermore, there’s no standard of diagnosis among professionals.
In rare cases, shoulder pain can indicate a serious medical problem — such as a heart attack — requiring immediate attention.
If you suffered direct trauma to the shoulder, or experience dizziness, double vision, difficulty speaking/swallowing, direct trauma, or unexplained weight loss accompanied by shoulder pain, seek immediate medical attention.